
Anyone following the world of health information technology (HIT) over the past decade knows there’s been tremendous work behind the scenes to advance interoperability and data sharing. Our efforts are finally coming to fruition as we move beyond the era of static document sharing into a new era of more intelligent data usability.
This is important because adoption will only increase when the data that clinicians need is quickly and easily accessible at the point of care. As an Internist MD and CMO myself, I know that physicians don’t have the time or cognitive bandwidth to parse through massive documents in search of the data they need, and I’m proud that my organization has aligned with MEDITECH to develop more intelligent forms of interoperability.
In this blog I’d like to provide an update on the most important work taking place in the industry today, clear up some confusion around key concepts and initiatives, and introduce some exciting work that’s in process. I’ll begin with the biggest and most important initiative underway — TEFCA. But first, I encourage you to take a moment to study the image below to familiarize yourself with some common terminology.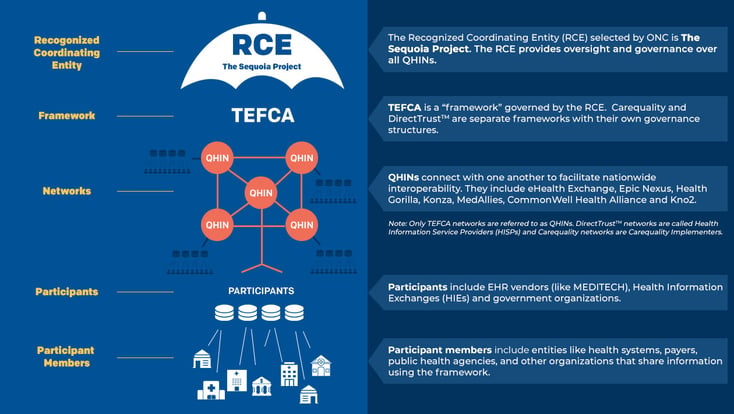
TEFCA
The Trusted Exchange Framework and Common Agreement (TEFCA) was a requirement of the 2016 21st Century Cures Act. TEFCA-designated Qualified Health Information Networks (QHINs) are designed to become the “on ramp” for all electronically accessible health information without special effort on the part of the user. The big news on the TEFCA front is that this requirement is now a reality. The first five QHINs were designated by ONC in December of 2023: eHealth Exchange, Epic Nexus, Health Gorilla, Konza and MedAllies. Earlier this month (February 2024) two additional QHINs were designated: CommonWell Health Alliance and Kno2.
TEFCA, DirectTrustTM and Carequality (on which TEFCA is based) are “Frameworks” that share certain characteristics:
- A common set of data sharing policies and legal terms for the networks operating under them
- Technical standards by which exchange actually happens (Implementation Guides / SOPs)
- Technical means of identifying trusted endpoints (directory)
- A process for onboarding and monitoring to ensure participants adhere to technical standards
- Governance to review and update all the above on a regular basis
- All have networks operating within the framework guidance and rules
Frameworks and Networks
TEFCA networks are called QHINs, Carequality networks are referred to as Carequality Implementers, and DirectTrustTM networks are designated as Health Information Service Providers (HISPs). MedAllies has developed and operates networks under all three frameworks and is a preferred MEDITECH vendor for Direct, a protocol that enables participants to send authenticated, encrypted health information to known and trusted recipients.
|
It is important to note that interoperable exchanges do not cross networks regulated by different frameworks. For example, an organization sending a message via Direct will not be received through a Carequality network into a recipient EHR. |
For example, both CommonWell and eHealth Exchange are Networks that have drawn different types of participants. CommonWell has attracted multiple EHR vendors while eHealth Exchange has engaged numerous Health Information Exchanges (HIEs) and Government organizations. That being said, in order to be able to exchange outside of their participating organizations in their Networks, they need to become Carequality Implementers. For example: CommonWell participants can readily exchange with the EHR vendor healthcare organizations within CommonWell, but to exchange with non-CommonWell EHR vendors they would need to subscribe to CommonWell’s Carequality Network as well.
|
The vision for QHINs is that all healthcare constituents will have a TEFCA QHIN, thereby the TEFCA QHIN will serve as the single interoperability on-ramp. Think of TEFCA as the internet of healthcare data. |
In addition, it is anticipated that the QHINs will be able to perform both “push” and “pull” use cases (explained below) as well as having a national roadmap to FHIR at Scale, which will be available in all designated QHINs by 2024.
“Push” and “Pull” Use Cases
For those unfamiliar with “push” and “pull” use cases, think of the “push” use case as particularly useful for things like transitions of care. For example, when a provider refers a patient to another provider, or the patient is transferring to another facility, they can ensure that the appropriate information is “pushed” to the receiving provider/facility to ensure that the patient receives optimal care. Typically, documents are “pushed” over Direct Networks or HISPs.
“Pull” use cases include querying to receive information needed for a patient, such as emergency encounters in the ED or querying for information for the roster of patients with upcoming scheduled encounters to ensure all information is available and up to date.
Data Usability
While both "push" and "pull" based forms of data exchange will continue to be important and have their use cases, for those of you who are currently utilizing interoperability and are unhappy with the information that you receive (for any number of reasons), there is important work being done to make the data sent and received more usable.
USCDI
The United States Core Data for Interoperability (USCDI), sponsored by ONC, is the standards body driving the data that Certified EHR (CEHRT) systems must be able to document and exchange as discrete, machine readable data to achieve certification. The process for proposing enhancements (and commenting on proposed enhancements) is transparent and open to the public, and an updated version is created with each cycle. As new versions are created, EHR vendors must include the most recent version of USCDI to remain certified. I know that MEDITECH is committed to updating the supported USCDI version annually, regardless of whether they are formally required to by regulation, which is no small feat! I empathize with EHR vendors like MEDITECH, who face a moving target as the USCDI continually enhances the required discrete data elements that must be included in CEHRT systems, but this kind of evolution is essential for advancing interoperability and thereby enhancing patient care.
But while the USCDI is helpful for defining the set of data elements that must be exchanged, that doesn't mean that this information can be easily understood and used in meaningful ways. To do that, we need to also make it usable for the data recipients.
Sequoia’s Data Usability Workgroup and Taking Root Movement
The Sequoia Project, which is the Recognized Coordinating Entity (RCE) for TEFCA, is dedicated to the success of interoperability. To that end, they built upon the work of the Carequality-CommonWell Joint Document Content Workgroup and multiple standards organizations and, in October 2020, founded the Interoperability Matters: Data Usability Workgroup.
There is far more to interoperability than getting information from point A to point B. The Data Usability Workgroup (which currently comprises 391 organizations and 486 participants) has focused on ensuring that the data received is trustworthy and usable. Their Data Usability Workgroup Implementation Guide (DUIG) Version 1 was published in December of 2022 and focused on the following:
• Data provenance & traceability of changes
• Effective use of codes
• Reducing the impact of duplicates
• Data integrity, format and trust
• Data tagging / searchability
• Effective use of narrative for usability
The DUIG version 2 is currently being developed by the Workgroup.
|
"At MedAllies we believe so strongly in interoperable data usability that we have built in the capability for all of our networks to enhance the interoperable data that flows across our network to recipient organizations based on the specifications of the DUIG Version 1. We will be updating to the specifications of the DUIG Version 2 once it has been published."
|

The Sequoia Taking Root Movement takes data usability to the next level. MedAllies is both an active member of the movement as well as a sponsor — the highest level of membership. MEDITECH is also a supporter. The movement is designed to promote development adoption of the DUIG.
There are 3 levels of Taking Root participation, which you can find on the organization’s website. These include:
Supporter: Pledges to support the data usability movement as a member of the interoperability community and the data usability community of practice. Invited to participate in a workgroup to aid in the development V2.0 of the Data Usability Guide.
Implementer: Pledges to implement the Data Usability Taking Root movement by adopting the V1.0 Data Usability Guide that promotes consistency across technologies. Implementers can choose their own implementation pathway and pace as outlined in the terms and conditions.
Sponsor: Pledges to co-sponsor the Data Usability Taking Root movement. Invests in the development of materials, toolkits, convenings, and outreach to launch and grow the movement on a national scale. Evangelizes the purpose and power of this work.
Interoperability Change Management
In addition to ensuring the data received is usable and trusted by the receiver, for interoperability to truly be adopted and embraced, everyone in the organization who has a role in sending, receiving, processing or reconciling the interoperable data must first understand how this will enhance both the ease of performing their jobs and improving their job performance — as well as their organization’s patient care. Then everyone needs to be thoroughly trained, screen by screen, on their EHR in order to perform their tasks.
|
There’s an expression in medicine, “Don’t practice until you get it right. Practice until you can’t get it wrong.” |
We will know that we have achieved our goals when healthcare constituents cannot imagine practicing medicine or performing their jobs without interoperable healthcare data exchange. Or, as I’ve heard MEDITECH’s Mike Cordeiro put it, “We'll know we've achieved true interoperability when we stop talking about it."
We still have work to do to get there but as the new year unfolds, we welcome the beginning of the next wave of healthcare interoperability — and we’re excited to work with MEDITECH to prioritize data usability.
Learn more about MEDITECH's robust suite of interoperability tools.




